Pharmacotherapeutic Group: Antineoplastic agent.
ATC Code: L01XC02.
Pharmacology: Pharmacodynamics: Mechanism of Action: Rituximab is a chimeric mouse/human monoclonal antibody that binds specifically to the transmembrane antigen CD20. This antigen is located on pre-B- and mature B-lymphocytes, but not on haemopoietic stem cells, pro-B-cells, normal plasma cells or other normal tissue. The antigen is expressed on >95% of all B-cell non-Hodgkin's lymphomas (NHLs). Following antibody binding, CD20 is not internalised or shed from the cell membrane into the environment. CD20 does not circulate in the plasma as a free antigen and, thus, does not compete for antibody binding.
Rituximab binds to the CD20 antigen on B-lymphocytes and initiates immunologic reactions that mediate B-cell lysis. Possible mechanisms of cell lysis include complement-dependent cytotoxicity (CDC), antibody-dependent cellular cytotoxicity (ADCC), and induction of apoptosis. Finally, in vitro studies have demonstrated that rituximab sensitises drug-resistant human B-cell lymphoma lines to the cytotoxic effects of some chemotherapeutic agents.
Peripheral B-cell counts declined to levels below normal following the first dose of MabThera/Rituxan. In patients treated for hematological malignancies, B-cell recovery began within 6 months of treatment and generally returning to normal levels within 12 months after completion of therapy, although in some patients this may take longer (see Clinical Trials: Experience from Clinical Trials in Hemato-Oncology under Adverse Reactions).
In patients with rheumatoid arthritis, the duration of peripheral B-cell depletion was variable. The majority of patients received further treatment prior to full B-cell repletion. A small proportion of patients had prolonged peripheral B-cell depletion lasting 2 years or more after their last dose of MabThera/Rituxan IV.
In GPA and MPA patients, peripheral blood CD19 B-cells depleted to less than 10 cells/μl following the first two infusions of rituximab and remained at that level in most patients through month 6.
Of 67 patients evaluated for human anti-mouse antibody (HAMA), none were positive. Of 356 non-Hodgkin's lymphoma patients evaluated for human anti-chimeric antibody (HACA) 1.1% (4 patients) were positive.
Clinical/Efficacy Studies: MabThera: Low-grade or FollicularNon-Hodgkin's Lymphoma: MabThera/Rituxan IV Monotherapy: Initial treatment, weekly for 4 doses: In the pivotal study, 166 patients with relapsed or chemoresistant low-grade or follicular B-cell NHL received 375 mg/m
2 of MabThera/Rituxan as an IV infusion weekly for four doses. The overall response rate (ORR) in the intent-to-treat (ITT) population was 48% (CI
95% 41% - 56%) with a 6% complete response (CR) and a 42% partial response (PR) rate. The projected median time to progression (TTP) for responding patients was 13.0 months.
In a subgroup analysis, the ORR was higher in patients with IWF B, C, and D histologic subtypes as compared to IWF A subtype (58% vs. 12%), higher in patients whose largest lesion was <5 cm versus >7 cm in greatest diameter (53% vs. 38%), and higher in patients with chemosensitive relapse as compared to chemoresistant (defined as duration of response <3 months) relapse (50% vs. 22%). ORR in patients previously treated with autologous bone marrow transplant (ABMT) was 78% vs. 43% in patients with no ABMT. Neither age, sex, lymphoma grade, initial diagnosis, presence or absence of bulky disease, normal or high LDH nor presence of extranodal disease had a statistically significant effect (Fisher's exact test) on response to MabThera/Rituxan IV.
A statistically significant correlation was noted between response rates and bone marrow involvement. Forty percent of patients with bone marrow involvement responded compared to 59% of patients with no bone marrow involvement (p=0.0186). This finding was not supported by a stepwise logistic regression analysis in which the following factors were identified as prognostic factors: histologic type, bcl-2 positivity at baseline, resistance to last chemotherapy and bulky disease.
Initial treatment, weekly for 8 doses: In a multi-center, single-arm study, 37 patients with relapsed or chemoresistant, low grade or follicular B-cell NHL received 375 mg/m
2 of MabThera/Rituxan as IV infusion weekly for eight doses. The ORR was 57% (CI
95% 41% - 73%; CR 14%, PR 43%) with a projected median TTP for responding patients of 19.4 months (range 5.3 to 38.9 months).
Initial treatment, bulky disease, weekly for 4 doses: In pooled data from three studies, 39 patients with relapsed or chemoresistant, bulky disease (single lesion ≥10 cm in diameter), low grade or follicular B-cell NHL received 375 mg/m
2 of MabThera/Rituxan as IV infusion weekly for four doses. The ORR was 36% (CI
95% 21% - 51%; CR 3%, PR 33%) with a median TTP for responding patients of 9.6 months (range 4.5 to 26.8 months).
Re-treatment, weekly for 4 doses: In a multi-center, single-arm study, 58 patients with relapsed or chemoresistant low grade or follicular B-cell NHL, who had achieved an objective clinical response to a prior course of MabThera/Rituxan IV were re-treated with 375 mg/m
2 of MabThera/Rituxan as IV infusion weekly for four doses. Three of the patients had received two courses of MabThera/Rituxan IV before enrollment and thus were given a third course in the study. Two patients were re-treated twice in the study. For the 60 re-treatments on study, the ORR was 38% (CI
95% 26% - 51%; 10% CR, 28% PR) with a projected median TTP for responding patients of 17.8 months (range 5.4 - 26.6). This compares favorably with the TTP achieved after the prior course of MabThera/Rituxan IV (12.4 months).
MabThera/Rituxan IV in Combination With Chemotherapy: Initial treatment: In an open-label randomized trial, a total of 322 previously untreated patients with follicular lymphoma were randomized to receive either CVP chemotherapy (cyclophosphamide 750 mg/m
2, vincristine 1.4 mg/m
2 up to a maximum of 2 mg on day 1, and prednisolone 40 mg/m
2/day on days 1-5) every 3 weeks for 8 cycles or MabThera/Rituxan IV 375 mg/m
2 in combination with CVP (R-CVP). MabThera/Rituxan IV was administered on the first day of each treatment cycle. A total of 321 patients (162 R-CVP, 159 CVP) received therapy and were analyzed for efficacy.
The median follow-up of patients was 53 months. R-CVP led to a significant benefit over CVP for the primary endpoint, time to treatment failure (27 months vs. 6.6 months, p< 0.0001, log-rank test). The proportion of patients with a tumour response (CR, CRu, PR) was significantly higher (p< 0.0001 Chi-Square test) in the R-CVP group (80.9%) than the CVP group (57.2%). Treatment with R-CVP significantly prolonged the time to disease progression or death compared to CVP, 33.6 months and 14.7 months, respectively (p< 0.0001, log-rank test). The median duration of response was 37.7 months in the R-CVP group and was 13.5 months in the CVP group (p< 0.0001, log-rank test). The difference between the treatment groups with respect to overall survival showed a strong clinical benefit (p=0.029, log-rank test stratified by center): survival rates at 53 months were 80.9% for patients in the R-CVP group compared to 71.1% for patients in the CVP group.
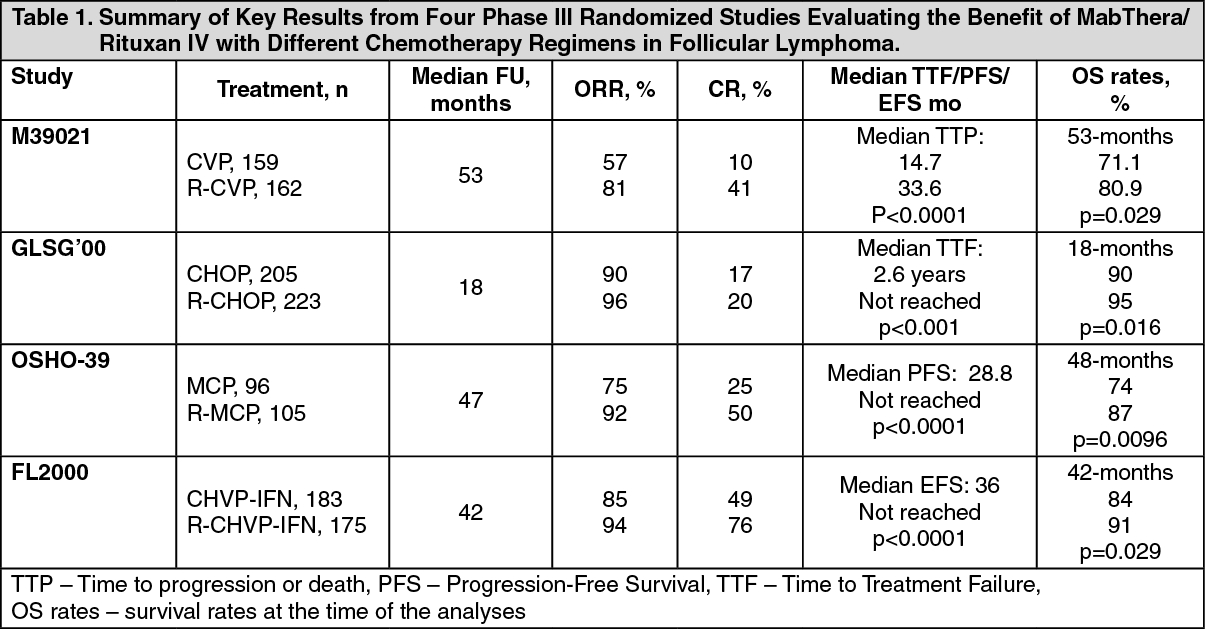
Results from three other randomized trials using MabThera/Rituxan IV in combination with chemotherapy regimen other than CVP (CHOP, MCP, CHVP/Interferon-α) also demonstrated significant improvements in response rates, time-dependent parameters as well as in overall survival. Key results from all four studies are summarized in Table 1 as follows. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
MabThera/Rituxan IV Maintenance Therapy: Previously untreated follicular NHL: In a prospective, open label, international, multi-center, phase III trial 1193 patients with previously untreated advanced follicular lymphoma received induction therapy with R-CHOP (n=881), R-CVP (n=268) or R-FCM (n=44), according to the investigators' choice. A total of 1078 patients responded to induction therapy, of which 1018 were randomized to MabThera/Rituxan IV maintenance therapy (n=505) or observation (n=513). The two treatment groups were well balanced with regards to baseline characteristics and disease status. MabThera/Rituxan IV maintenance treatment consisted of a single infusion of MabThera/Rituxan IV at 375 mg/ m
2 BSA given every 2 months until disease progression or for a maximum period of two years.
After a median observation time of 25 months from randomization, maintenance therapy with MabThera/Rituxan IV resulted in a clinically relevant and statistically significant improvement in the primary endpoint of investigator assessed progression-free survival (PFS) as compared to no maintenance therapy in patients with previously untreated follicular NHL. This improvement in PFS was confirmed by an independent review committee (IRC) (see Table 2 as follows).
Significant benefit from maintenance treatment with MabThera/Rituxan IV was also seen for the secondary endpoints event-free survival (EFS), time to next anti-lymphoma treatment (TNLT) time to next chemotherapy (TNCT) and overall response rate (ORR) (see Table 2 as follows).
The updated analysis corresponding to a median observation time of 73 months from randomization confirm the results of the primary analysis (see Table 2 as follows).
Click on icon to see table/diagram/image
Mabthera/Rituxan IV maintenance treatment provided consistent benefit in all subgroups tested: gender (male, femlae), age (<60 years, ≥60 years), FLIPI score (1,2 or 3), induction therapy (R-CHOP, R-CVP or R-FCM) and regardless of the quality of response to induction treatment (CR or PR).
Relapsed/Refractory follicular NHL: In a prospective, open label, international, multi-centre, phase III trial, 465 patients with relapsed/refractory follicular NHL were randomized in a first step to induction therapy with either CHOP (cyclophosphamide, doxorubicin, vincristine, prednisolone; n=231) or MabThera/Rituxan IV plus CHOP (R-CHOP, n=234). The two treatment groups were well balanced with regard to baseline characteristics and disease status. A total of 334 patients achieving a complete or partial remission following induction therapy were randomized in a second step to MabThera/Rituxan IV maintenance therapy (n=167) or observation (n=167). MabThera/Rituxan IV maintenance treatment consisted of a single infusion of MabThera/Rituxan IV at 375 mg/m
2 BSA given every 3 months until disease progression or for a maximum period of two years.
The final efficacy analysis included all patients randomized to both parts of the study. After a median observation time of 31 months for patients randomized to the induction phase, R-CHOP significantly improved the outcome of patients with relapsed/refractory follicular NHL when compared to CHOP (see Table 3 below).
Click on icon to see table/diagram/image
For patients randomized to the maintenance phase of the trial, the median observation time was 28 months from maintenance randomization. Maintenance treatment with MabThera/Rituxan IV led to a clinically relevant and statistically significant improvement in the primary endpoint, PFS, (time from maintenance randomization to relapse, disease progression or death) when compared to observation alone (p<0.0001 log-rank test). The median PFS was 42.2 months in the MabThera/Rituxan IV maintenance arm compared to 14.3 months in the observation arm. Using a cox regression analysis, the risk of experiencing progressive disease or death was reduced by 61% with MabThera/Rituxan IV maintenance treatment when compared to observation (95% CI; 45%-72%). Kaplan-Meier estimated progression-free rates at 12 months were 78% in the MabThera/Rituxan IV maintenance group vs. 57% in the observation group. An analysis of overall survival confirmed the significant benefit of MabThera/Rituxan IV maintenance over observation (p=0.0039 log-rank test). MabThera/Rituxan IV maintenance treatment reduced the risk of death by 56% (95% CI; 22%-75%).
The median time to new anti-lymphoma treatment was significantly longer with MabThera/Rituxan IV maintenance treatment than with observation (38.8 months vs. 20.1 months, p<0.0001 log-rank test). The risk of starting a new treatment was reduced by 50% (95% CI; 30%-64%). In patients achieving a CR/CRu (complete response unconfirmed) as best response during induction treatment, MabThera/Rituxan IV maintenance treatment significantly prolonged the median disease free survival (DFS) compared to the observation group (53.7 vs. 16.5 months, p=0.0003 log-rank test) (see Table 4 below). The risk of relapse in complete responders was reduced by 67% (95% CI; 39%-82%).
Click on icon to see table/diagram/image
The benefit of MabThera/Rituxan IV maintenance treatment was confirmed in all subgroups analyzed, regardless of induction regimen (CHOP or R-CHOP) or quality of response to induction treatment (CR or PR) (see Table 4). MabThera/Rituxan IV maintenance treatment significantly prolonged median PFS in patients responding to CHOP induction therapy (median PFS 37.5 months vs. 11.6 months, p<0.0001) as well as in those responding to R-CHOP induction (median PFS 51.9 months vs. 22.1 months, p=0.0071). MabThera/Rituxan IV maintenance treatment also provided a clinically meaningful benefit in terms of overall survival for both patients responding to CHOP and patients responding to R-CHOP in the induction phase of the study.
MabThera/Rituxan IV maintenance treatment provided consistent benefit in all subgroups tested: gender, age (≤60 years, >60 years), stage (III, IV), WHO performance status (0 vs. >0), B symptoms (absent, present), bone marrow involvement (no vs. yes), IPI (0-2 vs. 3-5), FLIPI score (0-1, vs. 2 vs. 3-5), number of extra-nodal sites (0-1 vs. >1), number of nodal sites (< 5 vs. ≥ 5), number of previous regimens (1 vs. 2), best response to prior therapy (CR/PR vs. NC/PD), haemoglobin (< 12 g/dL vs. ≥12 g/dL), β
2-microglobulin (< 3mg/L vs. ≥3 mg/L), LDH (elevated, not elevated) except for the small subgroup of patients with bulky disease.
Diffuse Large B-cell Non-Hodgkin's Lymphoma: In a randomized, open-label trial, a total of 399 previously untreated elderly patients (age 60 to 80 years) with diffuse large B-cell lymphoma received standard CHOP chemotherapy (cyclophosphamide 750 mg/m
2, doxorubicin 50 mg/m
2, vincristine 1.4 mg/m
2 up to a maximum of 2 mg on day 1, and prednisolone 40 mg/m
2/day on days 1 - 5) every 3 weeks for eight cycles, or MabThera/Rituxan IV 375 mg/m
2 plus CHOP (R-CHOP). MabThera/Rituxan IV was administered on the first day of the treatment cycle.
The final efficacy analysis included all randomized patients (197 CHOP, 202 R-CHOP), and had a median follow-up duration of approximately 31 months. The two treatment groups were well balanced in baseline characteristics and disease status. The final analysis confirmed that R-CHOP significantly increased the duration of event-free survival (the primary efficacy parameter, where events were death, relapse or progression of lymphoma, or institution of a new anti-lymphoma treatment) (p=0.0001). Kaplan Meier estimates of the median duration of event-free survival were 35 months in the R-CHOP arm compared to 13 months in the CHOP arm, representing a risk reduction of 41%. At 24 months, estimates for overall survival were 68.2% in the R-CHOP arm compared to 57.4% in the CHOP arm. A subsequent analysis of the duration of overall survival, carried out with a median follow-up duration of 60 months, confirmed the benefit of R-CHOP over CHOP treatment (p=0.0071), representing a risk reduction of 32%.
The analysis of all secondary parameters (response rates, progression-free survival, disease-free survival, duration of response) verified the treatment effect of R-CHOP compared to CHOP. The complete response rate after Cycle 8 was 76.2% in the R-CHOP group and 62.4% in the CHOP group (p=0.0028). The risk of disease progression was reduced by 46% and the risk of relapse by 51%.
In all patient subgroups (gender, age, age-adjusted IPI, Ann Arbor stage, ECOG, Beta 2 Microglobulin, LDH, Albumin, B-symptoms, Bulky disease, extranodal sites, bone marrow involvement), the risk ratios for event-free survival and overall survival (R-CHOP compared with CHOP) were less than 0.83 and 0.95; respectively. R-CHOP was associated with improvements in outcome for both high- and low-risk patients according to age-adjusted IPI.
Previously Untreated and Relapsed/Refractory Chronic Lymphocytic Leukaemia: In two open-label randomized trials, a total of 817 previously untreated patients and 552 patients with relapsed/refractory CLL were randomized to receive either FC chemotherapy (fludarabine 25 mg/m
2, cyclophosphamide 250 mg/m
2, days 1-3) every 4 weeks for 6 cycles or MabThera/Rituxan IV in combination with FC (R-FC). MabThera/Rituxan IV was administered at a dosage of 375 mg/m
2 during the first cycle one day prior to chemotherapy and at a dosage of 500 mg/m
2 on day 1 of each subsequent treatment cycle. A total of 810 patients (403 R-FC, 407 FC) in the first line study (see Table 5 and Table 6 as follows) and 552 patients (276 R-FC, 276 FC) for the relapsed/refractory study (see Table 7) were analyzed for efficacy.
In the first line study, after a median observation time of 20.7 months, the median progression-free survival (primary endpoint) was 40 months in the R-FC group and 32 months in the FC group (p<0.0001, log-rank test) (Table 5). The analysis of overall survival showed an improved survival in favour of the R-FC arm (p=0.0427, log-rank test). These results were confirmed with longer follow-up: after a median observation time of 48.1 months, the median PFS was 55 months in the R-FC group and 33 months in the FC group (p<0.0001, log-rank test) and overall survival analyses continued to show a significant benefit of R-FC treatment over FC chemotherapy alone (p=0.0319, log-rank test). The benefit in terms of PFS was consistently observed in most patient subgroups analyzed according to disease risk at baseline (i.e., Binet stages A-C) and was confirmed with longer follow-up (see Table 6).
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In the relapsed/refractory study, the median progression-free survival (primary endpoint) was 30.6 months in the R-FC group and 20.6 months in the FC group (p=0.002, log-rank test).
The benefit in terms of PFS was observed in almost all patient subgroups analyzed according to disease risk at baseline. A slight but not significant improvement in overall survival was reported in the R-FC compared to the FC arm. (See Table 7.)
Click on icon to see table/diagram/image
Results from other supportive studies using MabThera/Rituxan IV in combination with other chemotherapy regimens (including CHOP, FCM, PC, PCM, bendamustine and cladribine) for the treatment of CLL patients have also demonstrated high overall response rates with promising PFS rates without adding relevant toxicity to the treatment.
MabThera/Rituxan IV 90-Minute Infusion Rate Study (U4391g): Previously Untreated Follicular Non-Hodgkin's Lymphoma and Diffuse Large B-cell Non-Hodgkin's Lymphoma: In a prospective, open-label, phase III, multicenter, single-arm trial, 363 patients with previously untreated DLBCL receiving 375 mg/m
2 MabThera/Rituxan IV plus CHOP chemotherapy, or previously untreated follicular NHL receiving MabThera/Rituxan IV 375 mg/m
2 plus CVP chemotherapy, were treated with a 90-minute infusion of MabThera/Rituxan IV to evaluate the safety of a 90-minute infusion. Patients with clinically significant cardiovascular disease were excluded from the study.
Patients were eligible to continue in the study if they did not experience a Grade 3 or 4 infusion-related adverse event with Cycle 1 (at the standard MabThera/Rituxan IV infusion rate) and had a circulating lymphocyte count ≤ 5000/mm
3 before Cycle 2. Continuing patients received their Cycle 2 MabThera/Rituxan IV infusion as follows: 20% of the total dose given in the first 30 minutes and the remaining 80% of the total dose given over the next 60 minutes. Patients who tolerated the first 90-minute MabThera/Rituxan IV infusion (Cycle 2) continued to receive subsequent MabThera/Rituxan IV infusions at the 90-minute infusion rate for the remainder of the treatment regimen (through Cycle 6 or Cycle 8).
The primary endpoint of the study was the development of Grade 3 or 4 infusion-related toxicities (targeted adverse event) in patients who received MabThera/Rituxan IV by 90-minute infusion in Cycle 2.
The rate of Grade 3 and 4 IRRs on the day of and/or the day after the 90-minute MabThera/Rituxan IV infusion at Cycle 2 was 1.1% (95% CI [0.3%, 2.8%]). The rate of Grade 3 and 4 IRRs at any cycle (Cycles 2 to 8) at the 90-minute infusion rate was 2.8% (95% CI [1.3%, 5.0%]) (see Table 8). No acute fatal infusion related reactions were observed (see Clinical Trials under Adverse Reactions).
Click on icon to see table/diagram/image
MabThera SC: Previously Untreated Follicular Non-Hodgkin's Lymphoma BO22334 (SABRINA): A two-stage phase III, international, multicenter, randomized, controlled, open-label study was conducted in patients with previously untreated follicular lymphoma, to investigate the non-inferiority of the pharmacokinetic profile, together with efficacy and safety of MabThera/Rituxan SC in combination with CHOP or CVP vs. MabThera/Rituxan IV in combination with CHOP or CVP followed by MabThera/Rituxan maintenance therapy.
The objective of the first stage was to establish the MabThera/Rituxan SC dose that resulted in comparable rituximab serum C
trough levels compared with MabThera/Rituxan IV when given as part of induction treatment every 3 weeks for 8 cycles (see Pharmacology: Pharmacokinetics: Distribution under Actions). Stage 1 enrolled previously untreated patients with CD20-positive, follicular lymphoma (FL) Grade 1, 2 or 3a (n=127). Patients with a response at the end of induction therapy received maintenance therapy with the corresponding formulation (intravenous or subcutaneous) used in the induction treatment, every 8 weeks for 24 months.
The objective of Stage 2 was to provide additional efficacy and safety data for MabThera/Rituxan SC compared with MabThera/Rituxan IV using the 1400 mg subcutaneous dose established in Stage 1. Previously untreated patients with CD20-positive, follicular lymphoma Grade 1, 2 or 3a (n=283) were enrolled in Stage 2.
The overall study design was identical across Stage 1 and Stage 2. Patients were randomized into the following two treatment groups: MabThera/Rituxan SC arm (n=205): 1st cycle MabThera/Rituxan IV plus 7 cycles of MabThera/Rituxan SC in combination with up to 8 cycles of CHOP or CVP chemotherapy, administered every 3 weeks. MabThera/Rituxan IV was given at the standard dose of 375 mg/m
2. MabThera/Rituxan SC was given at a fixed dose of 1400 mg. Patients achieving at least partial response (PR) at the end of induction treatment were entered on to MabThera/Rituxan SC maintenance therapy administered once every 8 weeks for 24 months.
MabThera/Rituxan IV arm (n=205): 8 cycles of MabThera/Rituxan IV in combination with up to 8 cycles of CHOP or CVP chemotherapy administered every 3 weeks. MabThera/Rituxan IV was given at the standard dose of 375 mg/m
2. Patients achieving at least PR at the end of induction were entered on to MabThera/Rituxan IV maintenance therapy administered once every 8 weeks for 24 months.
Overall response rate (ORR, comprising complete response [CR], unconfirmed response [CRu], and partial response [PR]) at the end of induction treatment was calculated using investigator assessment of response in the ITT population based on pooled data from Stages 1 and 2. Additionally, ORR and complete response rate (CRR, comprising CR and CRu) at the end of maintenance treatment and time-to-event endpoints (progression-free survival [PFS] and overall survival [OS]) were analyzed. Efficacy results are presented in Table 9 based on a median observation time of approximately 37 months. (See Table 9.)
Click on icon to see table/diagram/image
Exploratory analyses showed response rates among BSA, chemotherapy and gender subgroups were not notably different from the overall ITT population.
MabThera: Rheumatoid Arthritis: The efficacy of MabThera/Rituxan IV in rheumatoid arthritis has been demonstrated in three pivotal, phase III, randomized, placebo-controlled, double-blind, multi-center studies. Eligible patients had severe, active RA, diagnosed according to the criteria of the American College of Rheumatology (ACR). MabThera/Rituxan IV was administered as two IV infusions separated by an interval of 15 days. Each course was preceded by an IV infusion of 100 mg methylprednisolone. All patients received concomitant oral methotrexate. In addition, in Study WA17042, all patients received concomitant oral glucocorticoids on days 2 to 7 and on days 8 to 14 following the first infusion.
The retreatment criteria differed between the studies using one of two approaches: 'Treatment to Remission' whereby patients were treated no more frequently than every 6 months if not in DAS28 remission (i.e., DAS28 ESR ≥2.6) and 'Treatment as Needed' strategy ('Treatment PRN'), based on disease activity and/or return of clinical symptoms (swollen and tender joint counts ≥ 8) and treated no sooner than every 16 weeks.
Study WA17042 (REFLEX) included 517 patients that had experienced an inadequate response or intolerance to one or more tumour necrosis factor (TNF) inhibitor therapies (TNF-IR). The primary endpoint was the proportion of patients who achieved an ACR20 response at Week 24. Patients received 2 x 1000 mg MabThera/Rituxan IV or placebo. Patients were followed beyond Week 24 for long-term endpoints, including radiographic assessment at 56 weeks. During this time patients could receive further courses of MabThera/Rituxan IV under an open label extension study protocol. In the open-label protocol patients received further courses based on the 'Treatment PRN' criteria.
Study WA17045 (SERENE) included 511 patients that had experienced an inadequate response to methotrexate (MTX-IR) and had not received prior biologic therapy. The primary endpoint was the proportion of patients who achieved an ACR20 response at Week 24. Patients received placebo, 2 x 500 mg or 2 x 1000 mg MabThera/Rituxan IV infusion. Patients were followed beyond Week 24 for long-term endpoints and could receive further courses of MabThera/Rituxan IV based on the 'Treatment to Remission' criteria. An active dose comparison was made at Week 48.
Disease Activity Outcomes: In these studies, MabThera/Rituxan IV (2 x 1000 mg) significantly increased the proportion of patients achieving at least a 20% improvement in ACR score compared with patients treated with methotrexate alone (see Table 10). Across all development studies the treatment benefit was similar in patients independent of age, gender, body surface area, race, number of prior treatments or disease status. Patients seropositive for disease-related auto-antibodies (RF and/or anti-CCP) demonstrated consistently high efficacy compared to MTX alone across studies. Efficacy in seropositive patients was higher than that observed in seronegative patients in whom efficacy was modest.
Clinically and statistically significant improvement was also noted on all individual components of the ACR response (tender and swollen joint counts, patient and physician global assessment, disability index scores [HAQ], pain assessment and CRP [mg/dl]).
Click on icon to see table/diagram/image
Patients treated with MabThera/Rituxan IV had a significantly greater reduction in disease activity score (DAS28) than patients treated with methotrexate alone. A good to moderate EULAR response was achieved by significantly more MabThera/Rituxan IV treated patients compared to patients treated with methotrexate alone (see Table 11).
Click on icon to see table/diagram/image
Inhibition of Joint Damage: In Studies WA17042 and WA17047 structural joint damage was assessed radiographically and expressed as change in modified Total Sharp Score (TSS) and its components, the erosion score and joint space narrowing score.
Study WA17042 conducted in TNF-IR patients receiving MabThera/Rituxan IV in combination with methotrexate, demonstrated significantly less radiographic progression at 56 weeks than patients from the methotrexate alone group. A higher proportion of patients receiving MabThera/Rituxan IV also had no erosive progression over 56 weeks.
Study WA17047 conducted in methotrexate-naïve patients (755 patients with early RA of between 8 weeks to four years duration), assessed the prevention of structural joint damage as its primary objective (see Precautions). Patients received placebo, 2 x 500 mg or 2 x 1000 mg MabThera/Rituxan IV infusion. From Week 24 patients could receive further courses of MabThera/Rituxan IV (or placebo to Week 104) based on the 'Treatment to Remission' criteria. The primary endpoint of change in modified Total Sharp Score (TSS) demonstrated that only treatment with MabThera/Rituxan IV at a dose of 2 x 1000 mg in combination with methotrexate significantly reduced the rate of progression of joint damage (PJD) at 52 weeks compared with placebo + methotrexate (see Table 12). The reduction in PJD was driven mainly by a significant reduction in the change in Erosion Score.
Inhibition of the rate of progressive joint damage was also observed long-term. Radiographic analysis at 2 years in Study WA17042 demonstrated significantly reduced progression of structural joint damage in patients receiving MabThera/Rituxan IV (2 x 1000 mg) + methotrexate compared to methotrexate alone as well as a significantly higher proportion of patients with no progression of joint damage over the 2 year period.
Click on icon to see table/diagram/image
Quality of Life Outcomes: MabThera/Rituxan IV treated patients reported an improvement in all patient-reported outcomes (HAQ-DI, FACIT-Fatigue and SF-36 questionnaires). Significant reductions in disability index (HAQ-DI), fatigue (FACIT-Fatigue), and improvement in the physical health domain of the SF-36 were observed in patients treated with MabThera/Rituxan IV compared to patients treated with methotrexate alone. (See Tables 13 and 14.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Laboratory Evaluations: In rheumatoid factor (RF) positive patients, marked decreases were observed in rheumatoid factor concentrations following treatment with MabThera/Rituxan IV in all three studies (range 45-64%, Figure 1). (See Figure 1.)
Click on icon to see table/diagram/image
Plasma total immunoglobulin concentrations, total lymphocytes counts, and white cell counts generally remained within normal limits following MabThera/Rituxan IV treatment, with the exception of a transient drop in white cell counts over the first four weeks following therapy. Titers of IgG antigen specific antibody to mumps, rubella, varicella, tetanus toxoid, influenza and
streptococcus pneumococci remained stable over 24 weeks following exposure to MabThera/Rituxan IV in rheumatoid arthritis patients.
Effects of rituximab on a variety of biomarkers were evaluated in patients enrolled into a clinical study. This sub-study evaluated the impact of a single treatment course of rituximab on levels of biochemical markers, including markers of inflammation (Interleukin 6, C Reactive protein, Serum amyloid type A protein, Protein S100 isotypes A8 and A9), autoantibody (RF and anti-cyclic citrullinated peptide immunoglobulin) production and bone turnover (osteocalcin and procollagen 1 N terminal peptide (P1NP)). MabThera/Rituxan IV treatment, whether as monotherapy or in combination with methotrexate or cyclophosphamide reduced the levels of inflammatory markers significantly, relative to methotrexate alone, over the first 24 weeks of follow-up. Levels of markers of bone turnover, osteocalcin and P1NP, increased significantly in the rituximab groups compared to methotrexate alone.
Long-term Efficacy with Multiple Course Therapy: In clinical studies patients were retreated based on either a 'Treatment to Remission' or a 'Treatment PRN' strategy. Repeat courses of MabThera/Rituxan IV maintained or improved treatment benefit, irrespective of the treatment strategy (Treatment to Remission or Treatment PRN) (Figure 2). However, Treatment to Remission generally provided better responses and tighter control of disease activity as indicated by ACRn, DAS28-ESR and HAQ-DI scores over time. Patients treated PRN also experienced returning disease symptoms between courses, as evidenced by DAS28-ESR scores which were close to pre-treatment levels prior to each course (Table 15). (See Figure 2 and Table 15.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
120-minute Infusion Rate Study (ML25641): In a multi-center, open-label single-arm trial, 351 patients with moderate-to-severe, active RA who had an inadequate response to at least one tumor necrosis factor inhibitor and were receiving methotrexate, were to receive 2 courses of MabThera/Rituxan IV treatment. Patients who were naïve to prior MabThera/Rituxan IV therapy (n=306) and those who had received 1 to 2 prior courses of MabThera/Rituxan IV 6 to 9 months prior to baseline (n=45), were eligible for enrollment.
Patients received 2 courses of MabThera/Rituxan IV (2 x 1000 mg) + methotrexate treatment with the first course administered on Days 1 and 15 and the second course six months later on Days 168 and 182. The first infusion of the first course (Day 1 infusion) was administered over a 4.25 hour (255 minutes) period. The second infusion of the first course (Day 15 infusion) and both infusions in the second course (Day 168 and 182 infusions) were administered over a 2 hour (120 minutes) period. Any patient experiencing a serious IRR with any infusion was withdrawn from the study.
The primary objective of the study was to assess the safety of administering the second infusion of the first study course of MabThera/Rituxan IV over a 2 hour (120 minutes) period.
The incidence of IRRs at Day 15 was 6.5% (95% CI [4.1%-9.7%]) consistent with the rate observed historically. There were no serious IRRs observed. Data observed for the infusions on Days 168 and 182 (120-minute infusion) demonstrates a low incidence of IRRs, similar to the rate observed historically, with no serious IRRs occurring (see Clinical Trials under Adverse Reactions).
Adult Patients with Granulomatosis with Polyangiitis (Wegener's) (GPA) and Microscopic Polyangiitis (MPA): Adult Induction of Remission: A total of 197 patients with severe, active granulomatosis with polyangiitis (Wegener's) (GPA) and microscopic polyangiitis (MPA) were enrolled and treated in an active controlled, randomized, double-blind, multicenter, non-inferiority study. Patients were 15 years of age or older, diagnosed with severely, active granulomatosis with polyangiitis (Wegener's) (75% of patients) or microscopic polyangiitis (MPA) (24% of patients) according to the Chapel Hill Consensus Conference Criteria. One percent of patients had unknown GPA and MPA type).
Patients were randomized in a 1:1 ratio to receive either oral cyclophosphamide daily (2 mg/kg/day) for 3 to 6 months, followed by azathioprine or MabThera/Rituxan IV (375 mg/m
2) once weekly for 4 weeks. Patients in both arms received 1000 mg of pulse IV methylprednisolone (or another equivalent-dose glucocorticoid) per day for 1 to 3 days, followed by oral prednisone (1 mg/kg/day, not exceeding 80 mg/day). Prednisone tapering was to be completed by 6 months from the start of study treatment.
The primary outcome measure was achievement of complete remission at 6 months defined as a Birmingham Vasculitis Activity Score for Wegener's Granulomatosis (BVAS/WG) of 0, and off glucocorticoid therapy. The prespecified non-inferiority margin for the treatment difference was 20%. The study demonstrated non-inferiority of MabThera/Rituxan IV to cyclophosphamide for complete remission at 6 months (see Table 16). In addition, the complete remission rate in the MabThera/Rituxan IV arm was significantly greater than the estimated complete remission rate in patients with severe GPA and MPA not treated or treated only with glucocorticoids, based on historical control data.
Efficacy was observed both for patients with newly diagnosed GPA and MPA and for patients with relapsing disease.
Click on icon to see table/diagram/image
Adult Maintenance Treatment: A total of 117 patients (88 with GPA, 24 with MPA, and 5 with renal-limited ANCA-associated vasculitis) in disease remission were randomized to receive azathioprine (59 patients) or MabThera/Rituxan IV (58 patients) in this prospective, multi-center, controlled, open-label study. Eligible patients were 21 to 75 years of age and had newly diagnosed or relapsing disease in complete remission after combined treatment with glucocorticoids and pulse cyclophosphamide. Patients were ANCA-positive at diagnosis or during the course of their disease; had histologically confirmed necrotizing small-vessel vasculitis with a clinical phenotype of GPA/MPA, or renal limited ANCA-associated vasculitis; or both.
Remission-induction therapy included IV prednisone, administered as per the investigator's discretion, preceded in some patients by methylprednisolone pulses, and pulse cyclophosphamide until remission was attained after 4 to 6 months. At that time, and within a maximum of 1 month after the last cyclophosphamide pulse, patients were randomly assigned to receive either MabThera/Rituxan IV (two 500 mg IV infusions separated by two weeks (on Day 1 and Day 15) followed by 500 mg IV every 6 months for 18 months or azathioprine (administered orally at a dose of 2 mg/kg/day for 12 months, then 1.5 mg/kg/day for 6 months, and finally 1 mg/kg/day for 4 months (treatment discontinuation after these 22 months). Prednisone treatment was tapered and then kept at a low dose (approximately 5 mg per day) for at least 18 months after randomization. Prednisone dose tapering and the decision to stop prednisone treatment after month 18 were left at the investigator's discretion.
All patients were followed until month 28 (10 or 6 months, respectively, after the last MabThera/Rituxan IV infusion or azathioprine dose).
Pneumocystis jirovecii pneumonia prophylaxis was required for all patients with CD4+ T-lymphocyte counts less than 250 per cubic millimeter.
The primary outcome measure was the rate of major relapse at month 28.
Results: At month 28, major relapse (defined by the reappearance of clinical and/or laboratory signs of vasculitis activity ([BVAS] > 0) that could lead to organ failure or damage or could be life threatening) occurred in three patients (5%) in the MabThera/Rituxan IV group and 17 patients (29%) in the azathioprine group (p=0.0007). Adjusting for the stratification factor using Cox PH modeling, MabThera/Rituxan IV reduced the risk of major relapse by approximately 86% relative to azathioprine (hazard ratio [HR]: 0.14; 95% confidence interval [CI]: 0.04, 0.47). Minor relapses (not life threatening and not involving major organ damage) occurred in seven patients in the MabThera/Rituxan IV group (12%) and eight patients in the azathioprine group (14%).
The cumulative incidence rate curves showed that time to first major relapse was longer in patients with MabThera/Rituxan IV starting from Month 2 and was maintained up to Month 28 (Figure 3). (See Figure 3.)
Click on icon to see table/diagram/image
Note, patients were censored at Month 28 if they had no event.
Pediatric Patients with Granulomatosis with Polyangiitis (Wegener's) (GPA) and Microscopic Polyangiitis (MPA): Study WA25615 (PePRS) was a multicenter, open-label, single-arm, uncontrolled study in 25 pediatric patients (≥ 2 to < 18 years old) with active GPA/MPA. The median age of patients in the study was: 14 years (range: 6-17 years) and the majority of patients (20/25 [80%]) were female. A total of 19 patients (76%) had GPA and 6 patients (24%) had MPA at baseline. Eighteen patients (72%) had newly diagnosed disease upon study entry (13 patients with GPA and 5 patients with MPA) and 7 patients had relapsing disease (6 patients with GPA and 1 patient with MPA).
The study design consisted of an initial 6-month remission induction phase, and a minimum 18-month follow-up phase up to a maximum of 54 months (4.5 years). The remission induction regimen consisted of four once weekly IV infusions of MabThera/Rituxan at a dose of 375 mg/m
2 BSA, on study days 1, 8, 15 and 22 in combination with oral prednisolone or prednisone at 1 mg/kg/day (max 60 mg/day) tapered to 0.2 mg/kg/day minimum (max 10 mg/day) by month 6. After the remission induction phase, patients could receive subsequent MabThera/Rituxan IV infusions on or after month 6 to maintain remission and control disease activity. Patients were to receive a minimum of 3 doses of IV methylprednisolone (30mg/kg/day, not exceeding 1g/day) prior to the first MabThera/Rituxan IV infusion. If clinically indicated, additional daily doses (up to three), of IV methylprednisolone could be given.
All 25 patients completed all four once weekly IV infusions for the 6-month remission induction phase. A total of 24 out of 25 patients completed at least 18 months of follow-up.
The objectives of this study was to evaluate safety, PK parameters, and efficacy of MabThera/Rituxan IV in pediatric GPA/MPA patients (≥ 2 to < 18 years old). The efficacy objectives of the study were exploratory and principally assessed using the Pediatric Vasculitis Activity Score (PVAS). (See Table 17.)
Click on icon to see table/diagram/image
Cumulative Glucocorticoid dose (IV and Oral) by Month 6: A clinically meaningful decrease in median overall oral glucocorticoid was observed from week 1 (median = 45 mg prednisone equivalent dose [IQR: 35 - 60]) to month 6 (median = 7.5 mg [IQR: 4-10]), which was subsequently maintained at month 12 (median = 5 mg [IQR: 2-10]) and month 18 (median =5 mg [IQR: 1-5]).
Follow-Up Treatment: After the 6-month remission induction phase, patients who had not achieved remission or who had progressive disease or flare that could not be controlled by glucocorticoids alone received additional treatment for GPA/MPA, that could include MabThera/Rituxan IV and/or other therapies, at the discretion of the investigator.
Fourteen out of 25 patients (56%) received additional MabThera/Rituxan IV treatment at or post month 6, up to month 18. Five patients received four once weekly doses (375 mg/m
2) of MabThera/Rituxan IV approximately every 6 months; 5 patients received a single dose (375 mg/m
2) of MabThera/Rituxan IV every 6 months, and a further 4 patients received various other MabThera/Rituxan doses/regimens according to their treating physician. Of the 14 patients, 9 patients achieved PVAS remission by month 6 and sustained remission through month 18; 4 patients achieved remission between month 6 and 12 and sustained remission through month 18. One patient first achieved remission between month 12 and 18.
Pemphigus Vulgaris: The efficacy and safety of MabThera/Rituxan IV in combination with short-term low dose glucocorticoid (prednisone) therapy were evaluated in newly diagnosed patients with moderate to severe pemphigus (74 pemphigus vulgaris [PV] and 16 pemphigus foliaceus [PF]) in this randomized, open-label, controlled, multicenter study. Patients were between 19 and 79 years of age and had not received prior therapies for pemphigus. In the PV population, five (13%) patients in the MabThera/Rituxan IV group and three (8%) patients in the standard prednisone group had moderate disease and 33 (87%) patients in the MabThera/Rituxan IV group and 33 (92%) patients in the standard dose prednisone group had severe disease according to disease severity defined by Harman's criteria.
Patients were stratified by baseline disease severity (moderate or severe) and randomized 1:1 to receive either MabThera/Rituxan IV and low dose prednisone or standard dose prednisone. Patients randomized to the MabThera/Rituxan IV group received an initial intravenous infusion of 1000 mg MabThera/Rituxan IV on Study Day 1 in combination with 0.5 mg/kg/day oral prednisone tapered off over 3 months if they had moderate disease or 1 mg/kg/day oral prednisone tapered off over 6 months if they had severe disease, and a second intravenous infusion of 1000 mg on Study Day 15. Maintenance infusions of MabThera/Rituxan IV 500 mg were administered at months 12 and 18. Patients randomized to the standard dose prednisone group received an initial 1 mg/kg/day oral prednisone tapered off over 12 months if they had moderate disease or 1.5 mg/kg/day oral prednisone tapered off over 18 months if they had severe disease. Patients in the MabThera/Rituxan IV group who relapsed could receive an additional infusion of MabThera/Rituxan IV 1000 mg in combination with reintroduced or escalated prednisone dose.
Maintenance and relapse infusions were administered no sooner than 16 weeks following the previous infusion.
The primary objective for the study was complete remission (complete epithelialization and absence of new and/or established lesions) at month 24 without the use of prednisone therapy for two months or more (CRoff for ≥2 months). Other efficacy parameters included evaluation of severe and moderate relapses (severity as defined by Harman's criteria and relapse defined as the appearance of ≥ 3 new lesions a month that did not heal spontaneously within 1 week, or the extension of established lesions in a patient who had achieved disease control), evaluation of the total median cumulative dose of prednisone, and the median duration of complete remission off corticosteroid therapy.
Results: The study demonstrated superiority of MabThera/Rituxan IV and low dose prednisone over standard dose prednisone in achieving CRoff ≥ 2 months at month 24 in PV patients (see Table 17). Additionally, at month 24, the proportion of PV patients with CRoff ≥ 3 months was higher in the MabThera/Rituxan IV and low dose prednisone group compared to the standard dose prednisone group (34 patients [90%] vs. 9 patients [25%], p value <0.0001).
Click on icon to see table/diagram/image
MabThera/Rituxan IV was considered steroid-sparing based on the duration that PV patients were off glucocorticoid therapy and cumulative exposure to glucocorticoids in the MabThera/Rituxan IV group compared to the standard dose prednisone group.
Duration off Glucocorticoid Therapy: Of PV patients who responded at month 24, the median duration of CRoff ≥2 months in the MabThera/Rituxan IV group was 498.5 days compared to 125 days in the standard dose prednisone group.
Glucocorticoid Exposure: The median (min, max) cumulative prednisone dose at month 24 was 5800 mg (2304, 29303) in the MabThera/Rituxan IV group compared to 20520 mg (2409, 60565) in the standard dose prednisone group.
Severe or Moderate Relapses: At month 24, 9 (24%) PV patients in the MabThera/Rituxan IV group experienced at least one severe or moderate relapse vs. 18 (50%) PV patients in the standard dose prednisone group.
Immunogenicity: As with all therapeutic proteins, there is the potential for an immune response in patients treated with MabThera/Rituxan. The data reflects the number of patients whose test results were considered positive for antibodies to rituximab using an enzyme-linked immunosorbent assay (ELISA). Immunogenicity assay results may be influenced by several factors including assay sensitivity and specificity, sample handling, timing of sample collection, concomitant medicinal products and underlying disease. For these reasons, comparison of incidence of antibodies to rituximab with the incidence of antibodies in other studies or to other products may be misleading.
MabThera: Rheumatoid Arthritis: Approximately 10% of patients with rheumatoid arthritis tested positive for anti-drug antibodies (ADA) in the RA clinical studies. The emergence of ADA was not associated with clinical deterioration or with an increased risk of reactions to subsequent infusions in the majority of patients. The presence of ADA may be associated with worsening of infusion or allergic reactions after the second infusion of subsequent courses, and failure to deplete B cells after receipt of further treatment courses has been observed rarely.
Adult and Pediatric Patients with Granulomatosis with Polyangiitis (Wegener's) (GPA) and Microscopic Polyangiitis (MPA): Twenty-three percent (23/99) of MabThera/Rituxan IV-treated patients from the adult GPA and MPA induction of remission trial and 18% (6/34) of MabThera/Rituxan IV-treated patients in the maintenance therapy clinical trial developed ADA.
In the pediatric clinical trial, a total of 4/25 patients (16%) developed ADA during the overall study period. Limited data shows there was no trend observed in the adverse reactions reported in ADA positive patients.
There was no apparent trend or negative impact of the presence of ADA on safety or efficacy in the adult and pediatric GPA and MPA clinical trials.
Pemphigus Vulgaris: By 18 months, a total of 19/34 (56%) (14 treatment-induced and 5 treatment-enhanced) MabThera/Rituxan IV treated PV patients tested positive for ADA. There was no apparent negative impact of the presence of ADA on safety or efficacy in the PV clinical study.
MabThera SC: Data from the subcutaneous formulation development program indicate that the formation of anti-rituximab antibodies (HACAs) after SC administration is comparable with that observed after IV administration. In the SABRINA study (BO22334) the incidence of treatment-induced/enhanced anti-rituximab antibodies in the SC group was low and similar to that observed in the IV group (1.5% IV vs. 2% SC). The incidence of treatment-induced/enhanced anti-rHuPH20 antibodies was 8% in the IV group compared with 13% in the SC group, and none of the patients who tested positive for anti-rHuPH20 antibodies tested positive for neutralizing antibodies. The overall proportion of patients found to have anti-rHuPH20 antibodies remained generally constant over the follow-up period in both cohorts.
In the SAWYER study (BO25341) the incidence of treatment-induced/enhanced anti-rituximab antibodies was similar in the two treatment arms; 6.7% IV vs. 2.4% SC. The incidence of treatment-induced/enhanced anti-rHuPH20 antibodies, only measured in patients in the SC arm was 10.6%. None of the patients who tested positive for anti-rHuPH20 antibodies tested positive for neutralizing antibodies.
The clinical relevance of the development of anti-rituximab or anti-rHuPH20 antibodies after treatment with MabThera/Rituxan SC is not known. There was no impact of the presence of anti-rituximab or anti-rHuPH20 antibodies on safety or efficacy in both studies.
Pharmacokinetics: Absorption: MabThera: Not applicable.
MabThera SC: SparkThera (BP22333): MabThera/Rituxan at a fixed dose of 1400 mg was administered subcutaneously during maintenance, after at least one cycle of MabThera/Rituxan IV at a dose of 375 mg/m
2, in FL patients who had previously responded to MabThera/Rituxan IV in induction. The predicted median C
max for the every two months regimen (q2m) for MabThera/Rituxan SC and the q2m regimen for MabThera/Rituxan IV were comparable at 201 and 209 µg/mL, respectively. Similarly for the every three months regimen (q3m) for MabThera/Rituxan SC and the q3m regimen for MabThera/Rituxan IV the predicted median C
max were comparable at 189 and 184 µg/mL, respectively. The median t
max in the MabThera/Rituxan SC group was approximately 3 days as compared to the t
max occuring at, or close to the end of the infusion for the MabThera/Rituxan IV group.
SABRINA (BO22334): MabThera/Rituxan at a fixed dose of 1400 mg was administered subcutaneously for 6 cycles during induction at 3-weekly intervals, following a first cycle of MabThera/Rituxan IV at a dose of 375 mg/m
2, in previously untreated FL patients in combination with chemotherapy. The serum rituximab C
max at Cycle 7 was similar between the two treatment arms, with geometric mean (CV%) values of 250.63 (19.01) μg/mL and 236.82 (29.41) μg/mL for MabThera/Rituxan IV and MabThera/Rituxan SC, respectively with the resulting geometric mean ratio (C
max, SC/C
max, IV) of 0.941 (90% CI: 0.872, 1.015).
Based on a population pharmacokinetic analysis an absolute bioavailability of 71.0% (95%CI: 70.0 - 72.1) was estimated.
Distribution: Non-Hodgkin's Lymphoma:
MabThera: Based on a population pharmacokinetic analysis in 298 NHL patients who received single or multiple infusions of MabThera/Rituxan IV as a single agent or in combination with CHOP therapy, the typical population estimates of nonspecific clearance (CL
1), specific clearance (CL
2) likely contributed by B cells or tumour burden, and central compartment volume of distribution (V
1) were 0.14 L/day, 0.59 L/day, and 2.7 L, respectively. The estimated median terminal elimination half-life of rituximab was 22 days (range, 6.1 to 52 days). Baseline CD19-positive cell counts and size of measurable tumour lesions contributed to some of the variability in CL
2 of rituximab in data from 161 patients given 375 mg/m
2 as an IV infusion for 4 weekly doses. Patients with higher CD19-positive cell counts or tumour lesions had a higher CL
2. However, a large component of inter-individual variability remained for CL
2 after correction for CD19-positive cell counts and tumour lesion size. V
1 varied by body surface area (BSA) and CHOP therapy. This variability in V
1 (27.1% and 19.0%) contributed by the range in BSA (1.53 to 2.32 m
2) and concurrent CHOP therapy, respectively, were relatively small. Age, gender, race, and WHO performance status had no effect on the pharmacokinetics of rituximab. This analysis suggests that dose adjustment of rituximab with any of the tested covariates is not expected to result in a meaningful reduction in its pharmacokinetic variability.
MabThera/Rituxan IV at a dose of 375 mg/m
2 was administered as an IV infusion at weekly intervals for 4 doses to 203 patients with NHL naive to rituximab. The mean C
max following the fourth infusion was 486 µg/mL (range, 77.5 to 996.6 µg/mL). The peak and trough serum levels of rituximab were inversely correlated with baseline values for the number of circulating CD19 positive B-cells and measures of disease burden. Median steady-state serum levels were higher for responders compared with non-responders. Serum levels were higher in patients with International Working Formulation (IWF) subtypes B, C, and D as compared with those with subtype A. Rituximab was detectable in the serum of patients 3 to 6 months after completion of last treatment.
MabThera/Rituxan IV at a dose of 375 mg/m
2 was administered as an IV infusion at weekly intervals for 8 doses to 37 patients with NHL. The mean C
max increased with each successive infusion, spanning from a mean of 243 µg/mL (range, 16-582 µg/mL) after the first infusion to 550 µg/mL (range, 171 1177 µg/mL) after the eighth infusion.
The pharmacokinetic profile of MabThera/Rituxan IV when administered as 6 infusions of 375 mg/m
2 in combination with 6 cycles of CHOP chemotherapy was similar to that seen with MabThera/Rituxan IV alone.
MabThera SC (1400 mg): SparkThera (BP22333): MabThera/Rituxan at a fixed dose of 1400 mg was administered subcutaneously during maintenance, after at least one cycle of MabThera/Rituxan IV at a dose of 375 mg/m
2, in FL patients who had previously responded to MabThera/Rituxan IV in induction. The predicted mean and geometric mean C
trough values at Cycle 2 were higher in the MabThera/Rituxan SC group than the MabThera/Rituxan IV group. The geometric mean values for the q2m regimen for MabThera/Rituxan SC and the q2m regimen for MabThera/Rituxan IV were 32.2 and 25.9 µg/mL, respectively and the q3m regimen for MabThera/Rituxan SC and the q3m regimen for MabThera/Rituxan IV were 12.1 and 10.9 µg/mL, respectively. Similarly, the predicted mean and geometric mean AUC
tau values at Cycle 2 were higher in the MabThera/Rituxan SC group compared with the MabThera/Rituxan IV group. The geometric mean for the q2m regimen for MabThera/Rituxan SC and the q2m regimen for MabThera/Rituxan IV were 5430 and 4012 µg•day/mL, respectively and the q3m regimen for MabThera/Rituxan SC and the q3m regimen for MabThera/Rituxan IV were 5320 and 3947 µg•day/mL, respectively.
SABRINA (BO22334): MabThera/Rituxan at a fixed dose of 1400 mg was administered as a subcutaneous injection, in the abdomen, at 3-weekly intervals. Previously untreated patients with CD20+ FL Grade 1, 2, or 3a were randomized 1:1 to receive MabThera/Rituxan SC (first cycle MabThera/Rituxan IV at a dose of 375 mg/m
2 followed by 7 cycles of MabThera/Rituxan SC) or MabThera/Rituxan IV at a dose of 375 mg/m
2 (for 8 cycles) in combination with up to 8 cycles of CHOP or CVP chemotherapy administered every three weeks as part of induction treatment. The mean and geometric mean C
trough values at induction Cycle 7 (pre-dose Cycle 8) were higher among the MabThera/Rituxan SC group compared with the MabThera/Rituxan IV group. The geometric mean was 134.6 µg/mL for the MabThera/Rituxan SC group compared with 83.1 µg/mL for the MabThera/Rituxan IV group.
Similarly, the mean and geometric mean AUC values at induction Cycle 7 (pre-dose Cycle 8) were higher among the MabThera/Rituxan SC group than the MabThera/Rituxan IV group. The geometric mean AUC was 3778.9 µg•day/mL for the MabThera/Rituxan SC group compared with 2734.2 µg•day/mL for the MabThera/Rituxan IV group.
In a population pharmacokinetic analysis in FL patients who received single or multiple infusions of MabThera/Rituxan IV as a single agent or in combination with chemotherapy, the population estimates of nonspecific clearance (CL
1), initial specific clearance (CL
2) (likely contributed by B cells or tumour burden) and central compartment volume of distribution (V
1) were 0.194 L/day, 0.535 L/day, and 4.37 L, respectively. The estimated median terminal elimination half-life of MabThera/Rituxan SC was 29.7 days (range, 9.9 to 91.2 days).
In the final analysis dataset from 403 patients administered MabThera/Rituxan SC and/or IV in Studies BP22333 (277 patients) and BO22334 (126 patients) the mean (range) weight and BSA were 74.4 kg (43.9 to 130 kg) and 1.83 m
2 (1.34 to 2.48 m
2), respectively. Mean (range) age was 57.4 years (23 to 87 years). There were no differences between demographic and laboratory parameters for the two studies. However, the baseline B-cell counts were markedly lower in Study BP22333, than in Study BO22334, as patients in Study BP22333 entered the study having received a minimum of four cycles of MabThera/Rituxan IV in induction and at least one cycle of MabThera/Rituxan IV maintenance, whereas patients in Study BO22334 had not received MabThera/Rituxan prior to study enrollment. Data on baseline tumor load was available only for patients in Study BO22334.
BSA was identified as the main covariate. All clearance and volume parameters increased with the body size. Among other covariate dependencies, central volume increased with age and the absorption rate constant decreased with age (for patients aged > 60 years), but these age dependencies were shown to result in negligible changes in rituximab exposure. Anti-drug antibodies were detected in only 13 patients and did not result in any clinically relevant increase in clearance.
Chronic Lymphocytic Leukaemia:
MabThera: MabThera/Rituxan was administered as an IV infusion at a first-cycle dose of 375 mg/m
2 increased to 500 mg/m
2 each cycle for 5 doses in combination with fludarabine and cyclophosphamide in CLL patients. The mean C
max (n=15) was 408 µg/mL (range, 97 - 764 µg/mL) after the fifth 500 mg/m
2 infusion.
Rheumatoid Arthritis: Following two intravenous infusions of rituximab at a dose of 1000 mg, two weeks apart, the mean terminal half-life was 20.8 days (range, 8.58 to 35.9 days), mean systemic clearance was 0.23 L/day (range, 0.091 to 0.67 L/day), and mean steady-state distribution volume was 4.6 L (range, 1.7 to 7.51 L). Population pharmacokinetic analysis of the same data gave similar mean values for systemic clearance and half-life, 0.26 L/day and 20.4 days, respectively. Population pharmacokinetic analysis revealed that BSA and gender were the most significant covariates to explain inter-individual variability in pharmacokinetic parameters. After adjusting for BSA, male subjects had a larger volume of distribution and a faster clearance than female subjects. The gender-related pharmacokinetic differences are not considered to be clinically relevant and dose adjustment is not required.
The pharmacokinetics of rituximab were assessed following two IV doses of 500 mg and 1000 mg on Days 1 and 15 in four studies. In all these studies, rituximab pharmacokinetics were dose proportional over the limited dose range studied. Mean C
max for serum rituximab following first infusion ranged from 157 to 171 µg/mL for 2 x 500 mg dose and ranged from 298 to 341 µg/mL for 2 x 1000 mg dose. Following second infusion, mean C
max ranged from 183 to 198 µg/mL for the 2 x 500 mg dose and ranged from 355 to 404 µg/mL for the 2 x 1000 mg dose. Mean terminal elimination half life ranged from 15 to 16.5 days for the 2 x 500 mg dose group and 17 to 21 days for the 2 x 1000 mg dose group. Mean C
max was 16 to 19% higher following second infusion compared to the first infusion for both doses.
The pharmacokinetics of rituximab were assessed following two IV doses of 500 mg and 1000 mg upon re-treatment in the second course. Mean C
max for serum rituximab following first infusion was 170 to 175 µg/mL for 2 x 500 mg dose and 317 to 370 µg/mL for 2 x 1000 mg dose. C
max following second infusion was 207 µg/mL for the 2 x 500 mg dose and ranged from 377 to 386 µg/mL for the 2 x 1000 mg dose. Mean terminal elimination half-life after the second infusion, following the second course, was 19 days for 2 x 500 mg dose and ranged from 21 to 22 days for the 2 x 1000 mg dose. PK parameters for rituximab were comparable over the two treatment courses.
The pharmacokinetic parameters in the anti-TNF inadequate responder population, following the same dosage regimen (2 x 1000 mg, IV, 2 weeks apart), were similar with a mean maximum serum concentration of 369 µg/mL and a mean terminal half-life of 19.2 days.
Adult and Pediatric Granulomatosis with Polyangiitis (Wegener's) (GPA) and Microscopic Polyangiitis (MPA): The PK parameters in adult and pediatric patients with GPA/MPA receiving 375 mg/m
2 MabThera/Rituxan IV once weekly for four doses are summarized in Table 19. (See Table 19.)
Click on icon to see table/diagram/image
The PK parameters of rituximab in adult GPA / MPA patients appear similar to what has been observed in RA patients (see Pharmacology: Pharmacokinetics: Distribution under Actions).
Based on a population pharmacokinetic analysis in pediatric patients with GPA /MPA, the PK parameters of rituximab were similar to those in adults with GPA/MPA, once taking into account the BSA effect on clearance and volume parameters.
Metabolism: No text.
Elimination: See Pharmacology: Pharmacokinetics: Distribution under Actions.
Pharmacokinetics in Special Populations: Renal impairment: No pharmacokinetic data are available in patients with hepatic or renal impairment.
Hepatic impairment: No pharmacokinetic data are available in patients with hepatic impairment.
Pediatrics: The effect of body surface area on the pharmacokinetics of rituximab IV was assessed in a population pharmacokinetic analysis which included 9 children (≥ 6 years to < 12 years) and 16 adolescents (12 to < 18 years) with GPA/MPA. BSA was a significant covariate on rituximab pharmacokinetics (see Special Dosage Instructions under Dosage & Administration).
Toxicology: Preclinical Safety: Carcinogenicity: No text.
Genotoxicity: No text.
Impairment of fertility: No text.
Reproductive Toxicity: No text.
Other:
MabThera SC: The subcutaneous formulation contains recombinant human hyaluronidase (rHuPH20), an enzyme used to increase the dispersion and absorption of co-administered drugs when administered subcutaneously. Systemic absorption of rHuPH20 after subcutaneous administration is unlikely to occur. However, pharmacokinetic and toxicology studies in animals demonstrate reductions in foetal weight and increases in the number of resorptions following injection of rHuPH20 at maternal systemic exposure levels comparable to those that could occur after accidental bolus IV administration of a single vial of the MabThera/Rituxan SC formulation in humans, based on the most conservative assumptions possible. There is no evidence of dysmorphogenesis (i.e., teratogenesis) resulting from systemic exposure to rHuPH20.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image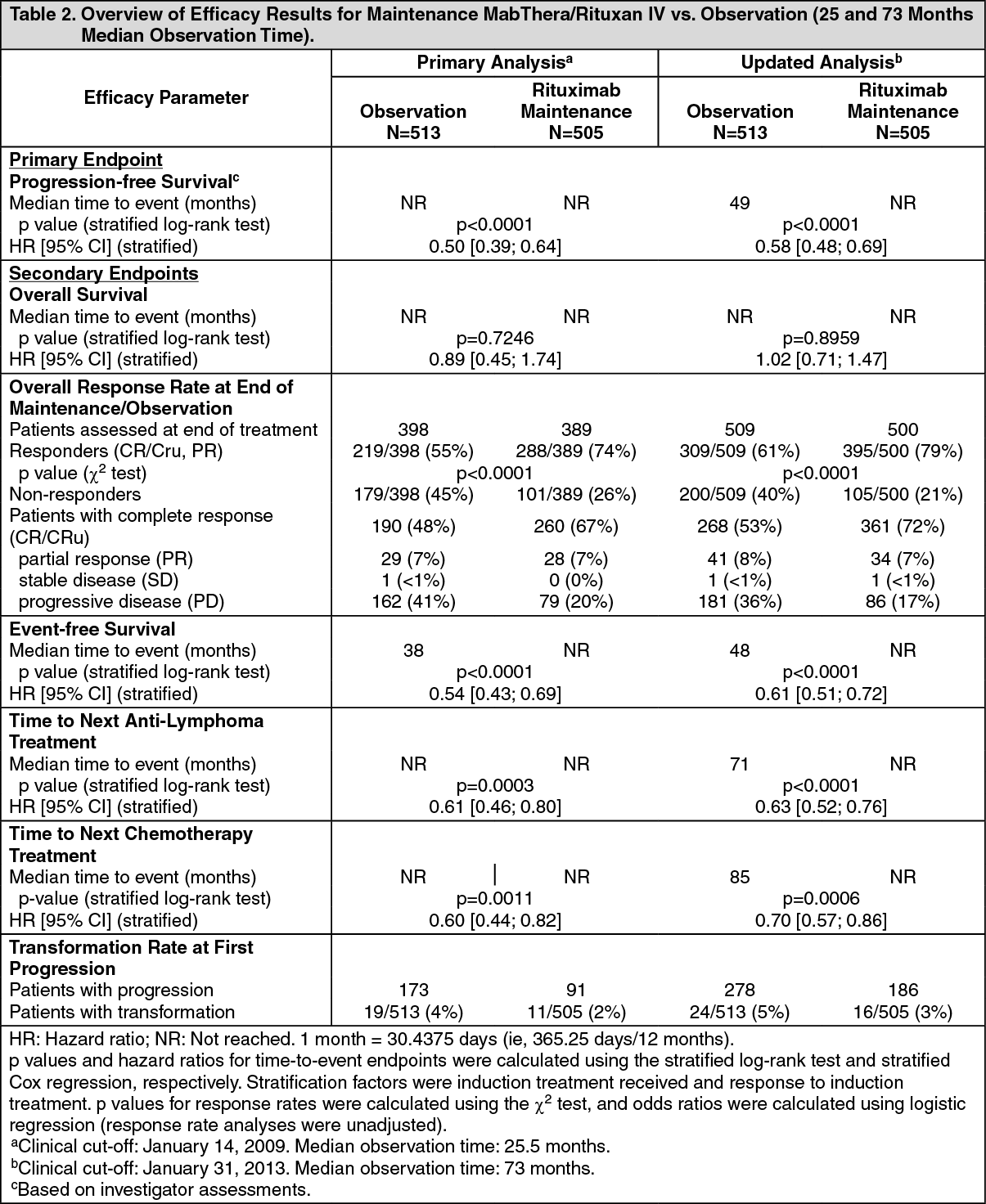 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image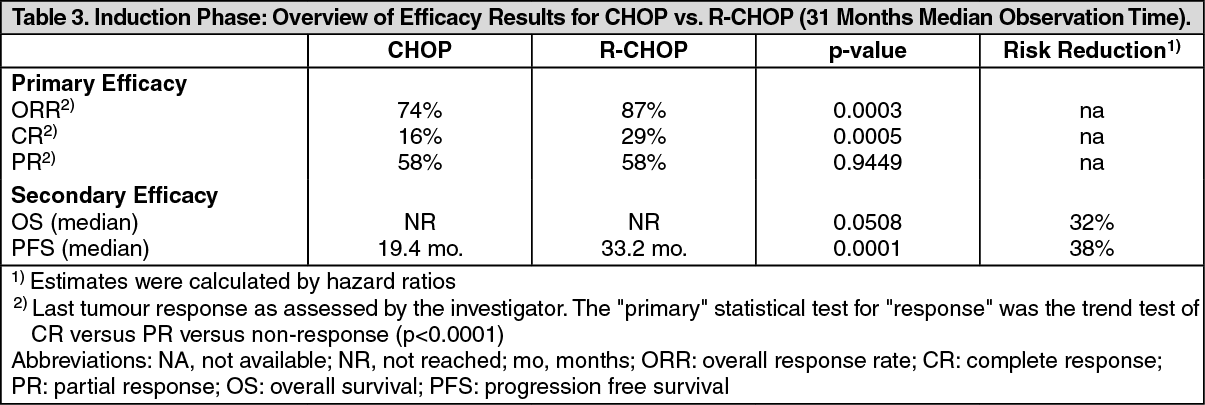 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image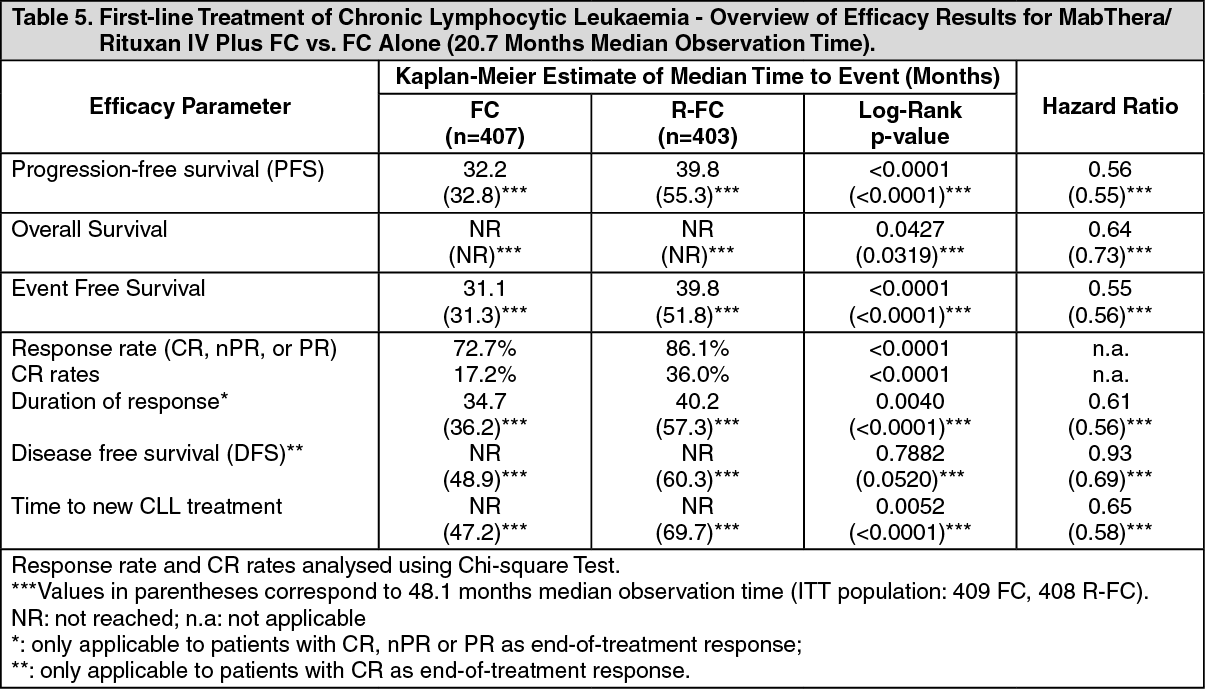 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image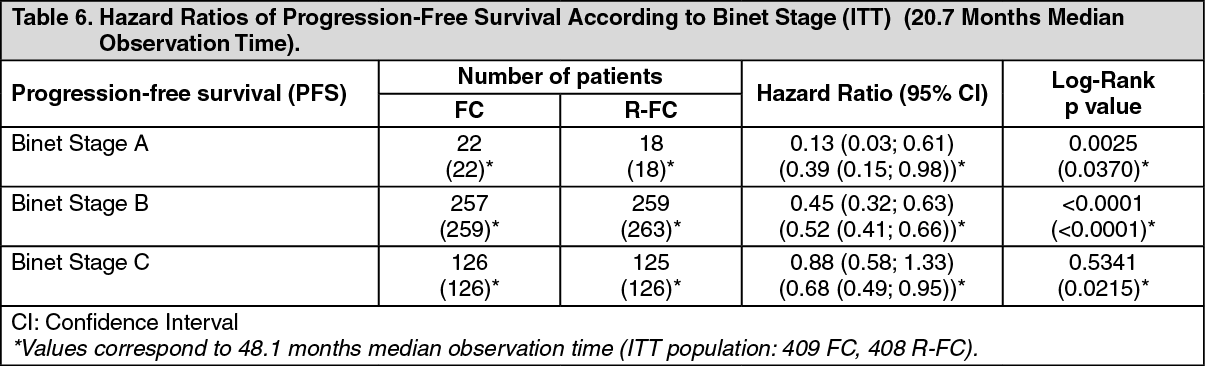 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image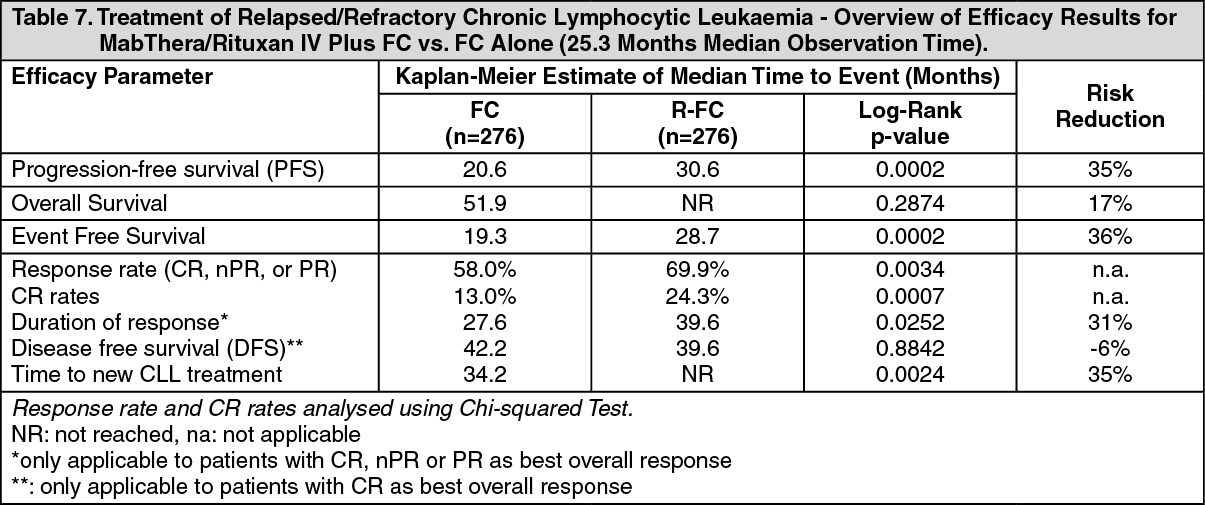 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image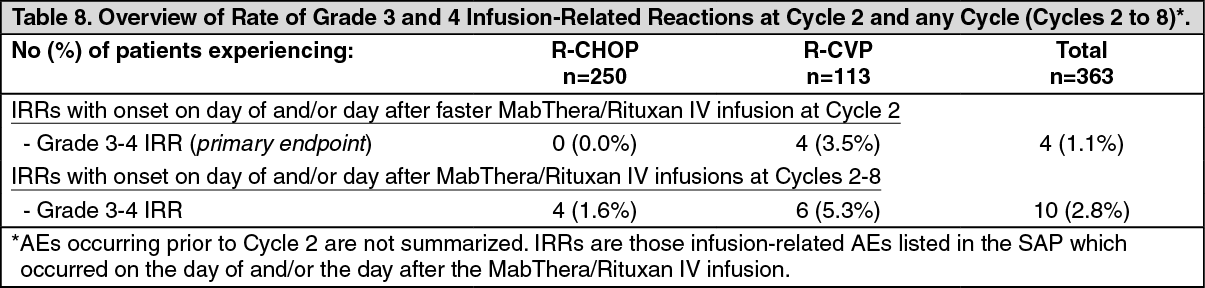 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image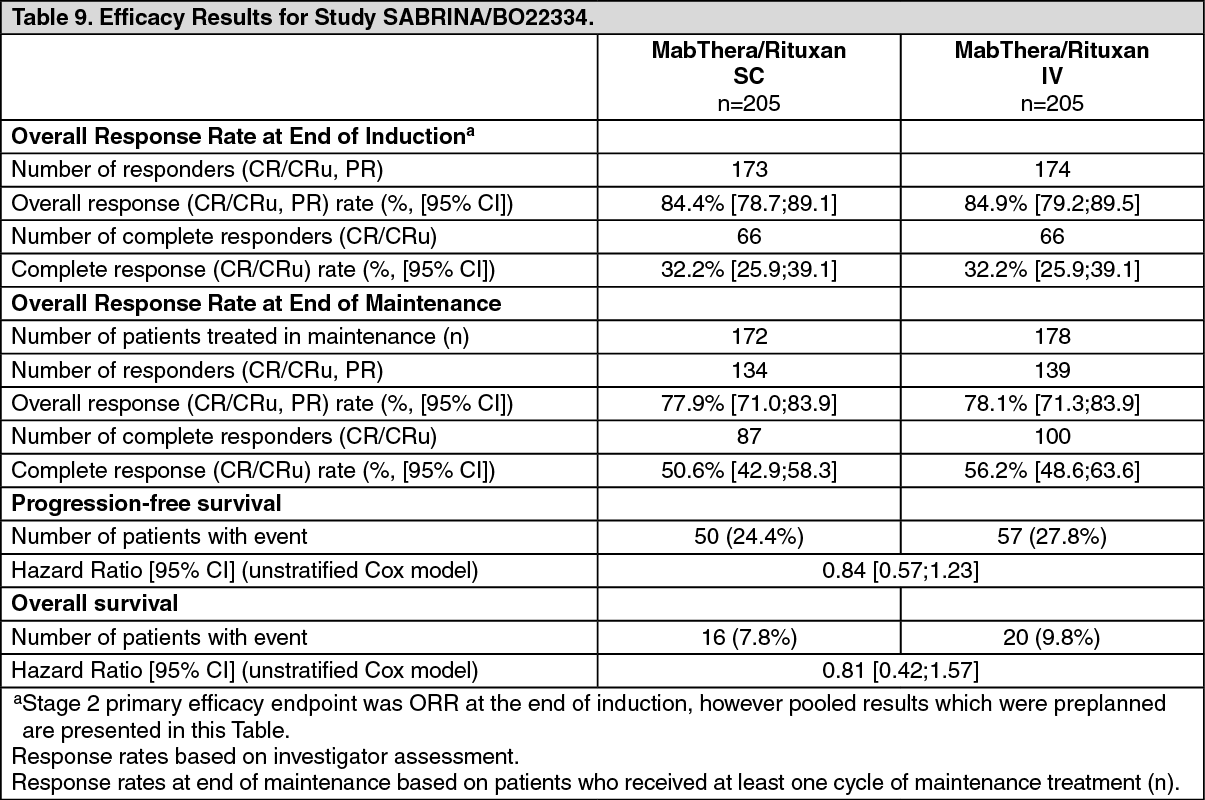 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image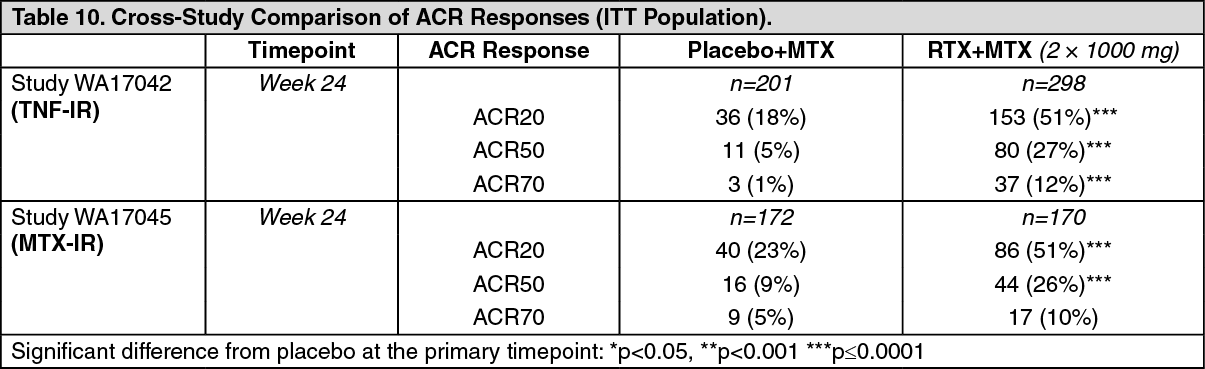 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image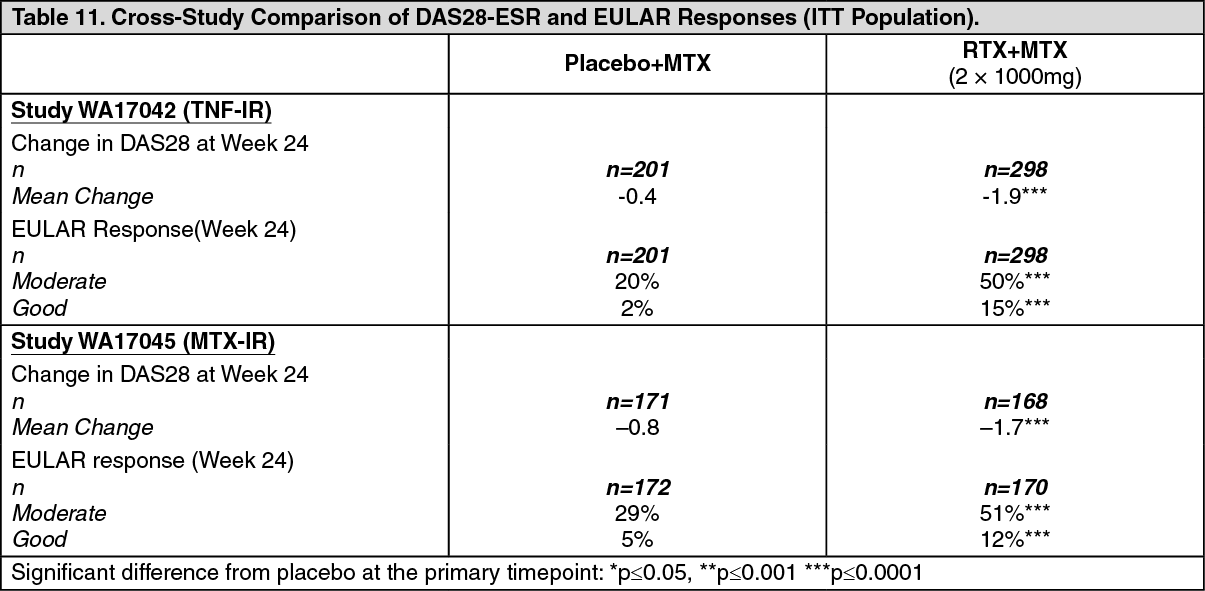 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image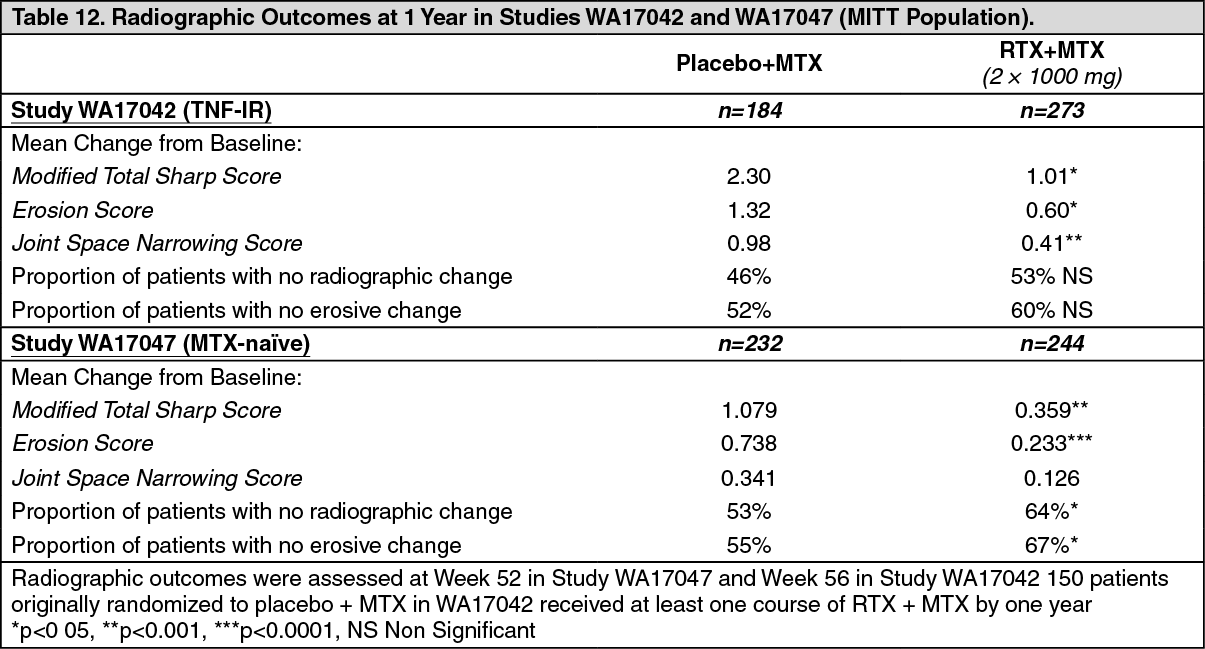 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image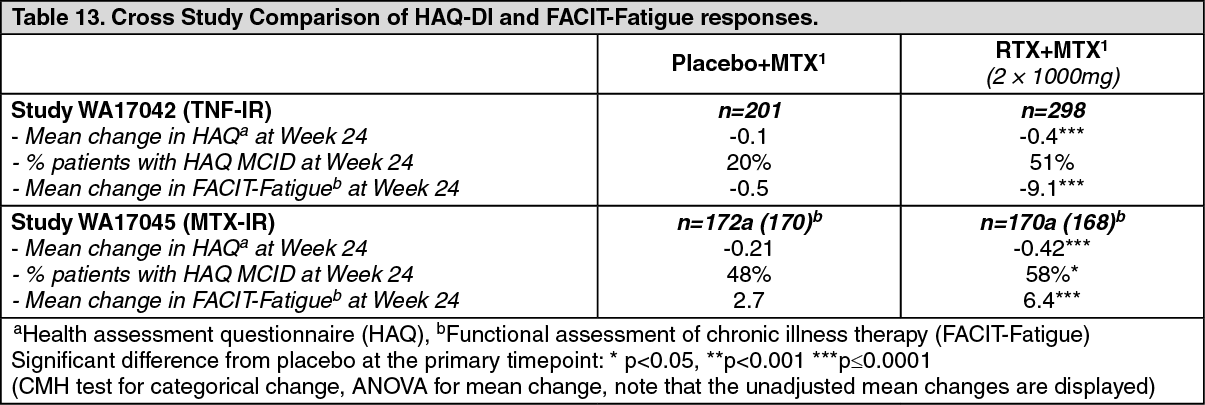 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image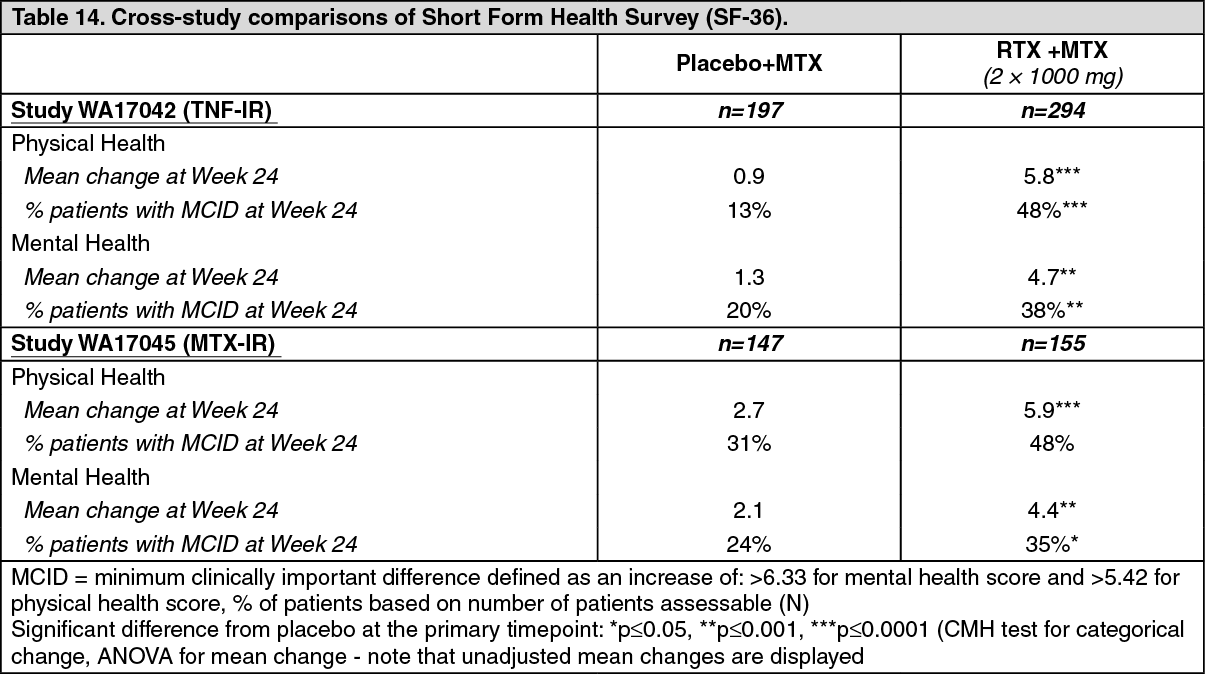 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image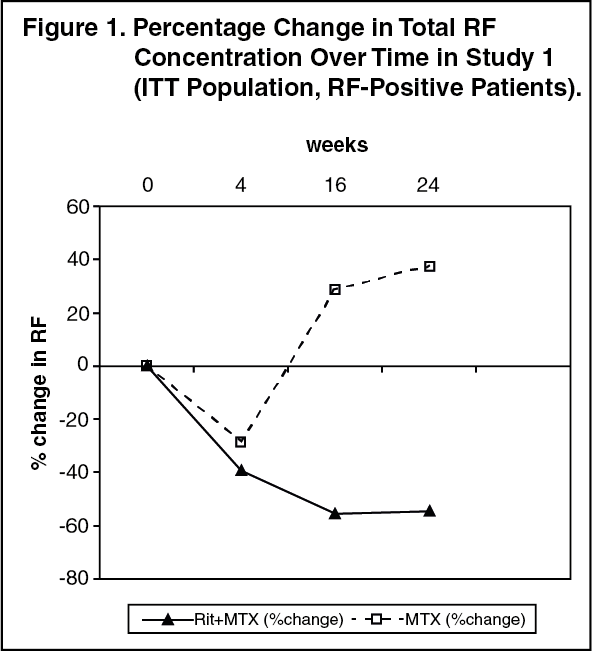 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image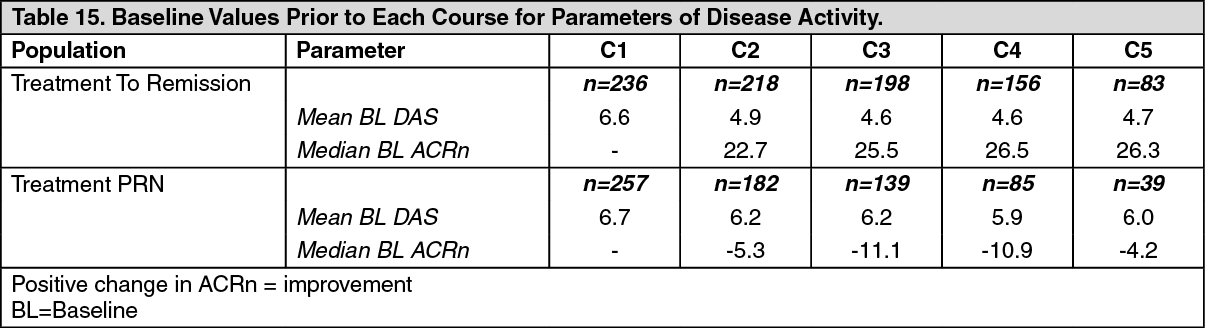 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image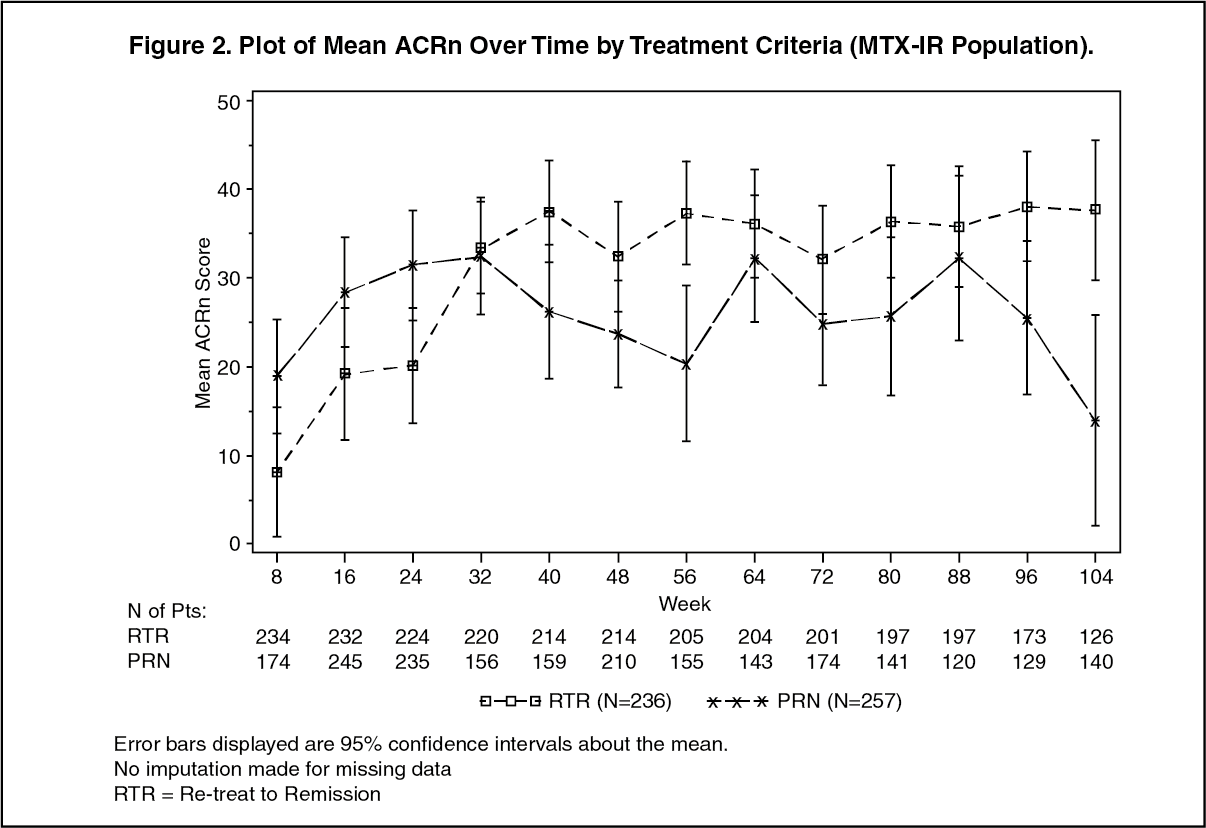 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image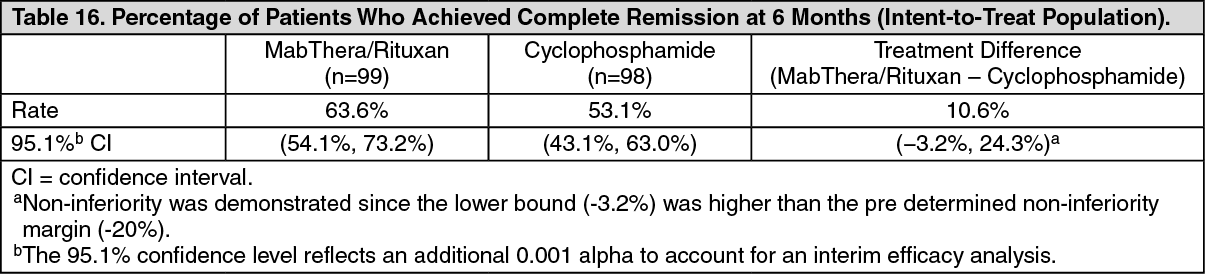 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image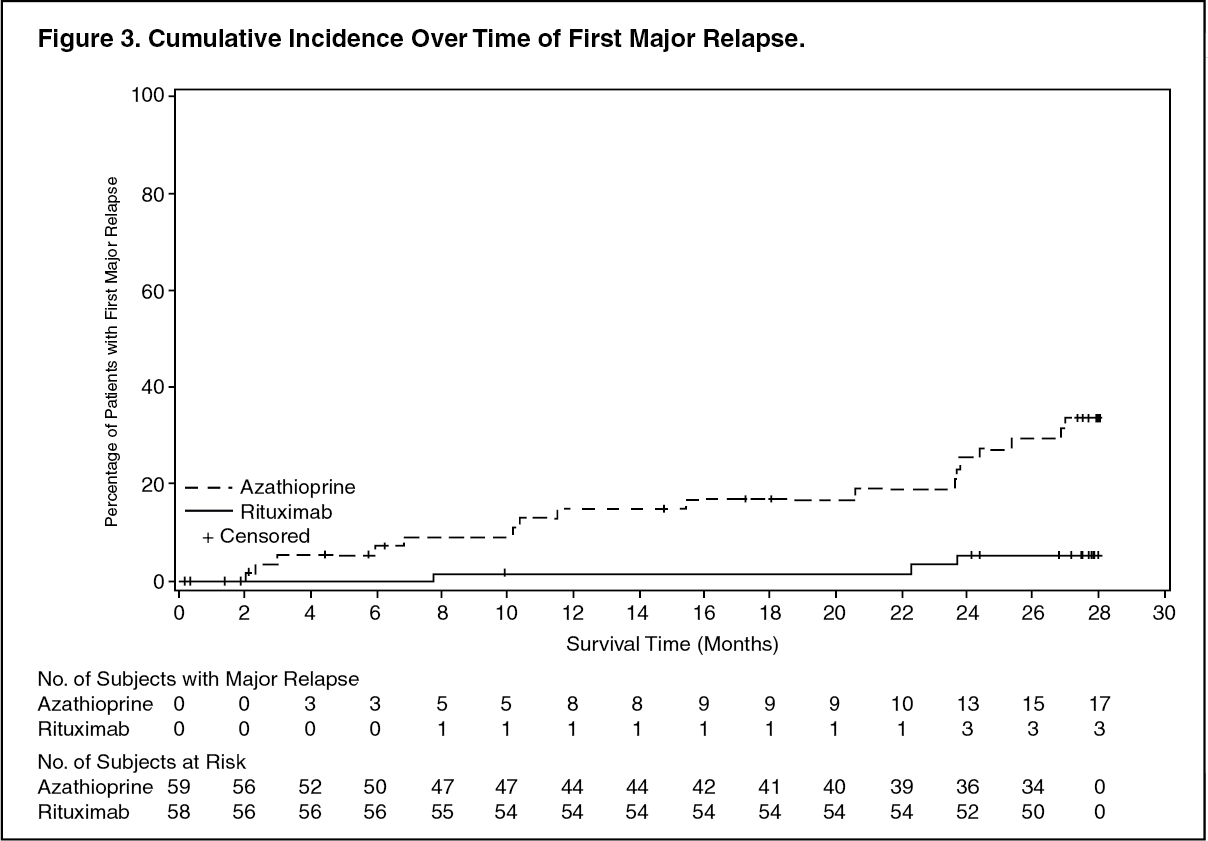 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image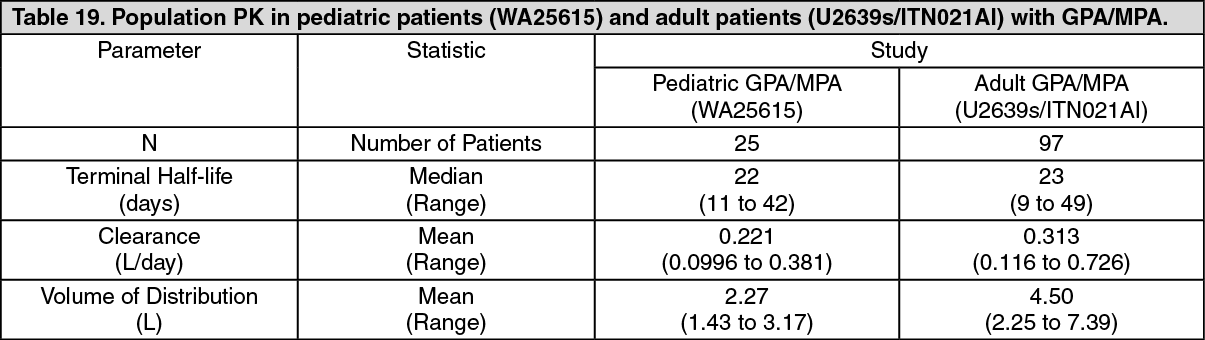 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
